every
day
counts
Alarm signs
Remind your patients to go to their doctor or podiatrist straight away if they notice any of these signs during their foot check:
- An ulcer
- A scratch
- A cut
- A blister
- Feel pain
- Swelling
- Redness
In the case of the presence of a wound or a blister, cut or scratch it is key to react early and appropriately to avoid serious complications and potential amputation.
Remind your patients what to do if they notice a problem
If they notice something wrong, it is very important to:
- Take the weight off the foot
- Contact their GP, podiatrist or nurse as soon as possible
- Go to their nearest out-of-hours healthcare service if their GP, podiatrist or nurse is not available
It is extremely important to react early and appropriately before it gets any worse – no matter how small the wound. A serious foot problem for some patients could lead to amputation in a short period of time.
It is very important to remember to keep the weight off the foot.
A key success factor to closing the wound and to avoiding complication such as infection, and a potential amputation is to react early. It is very important that your patients and you react early to close the wound.
every
step
matters
the sooner,
the better.
Making an appropriate referral
It is key to refer the diabetic patient with foot ulceration to the right person at the right time. Here are the international recommendations1 from D-FOOT International to assist you in the referral of your patients to specialised settings.
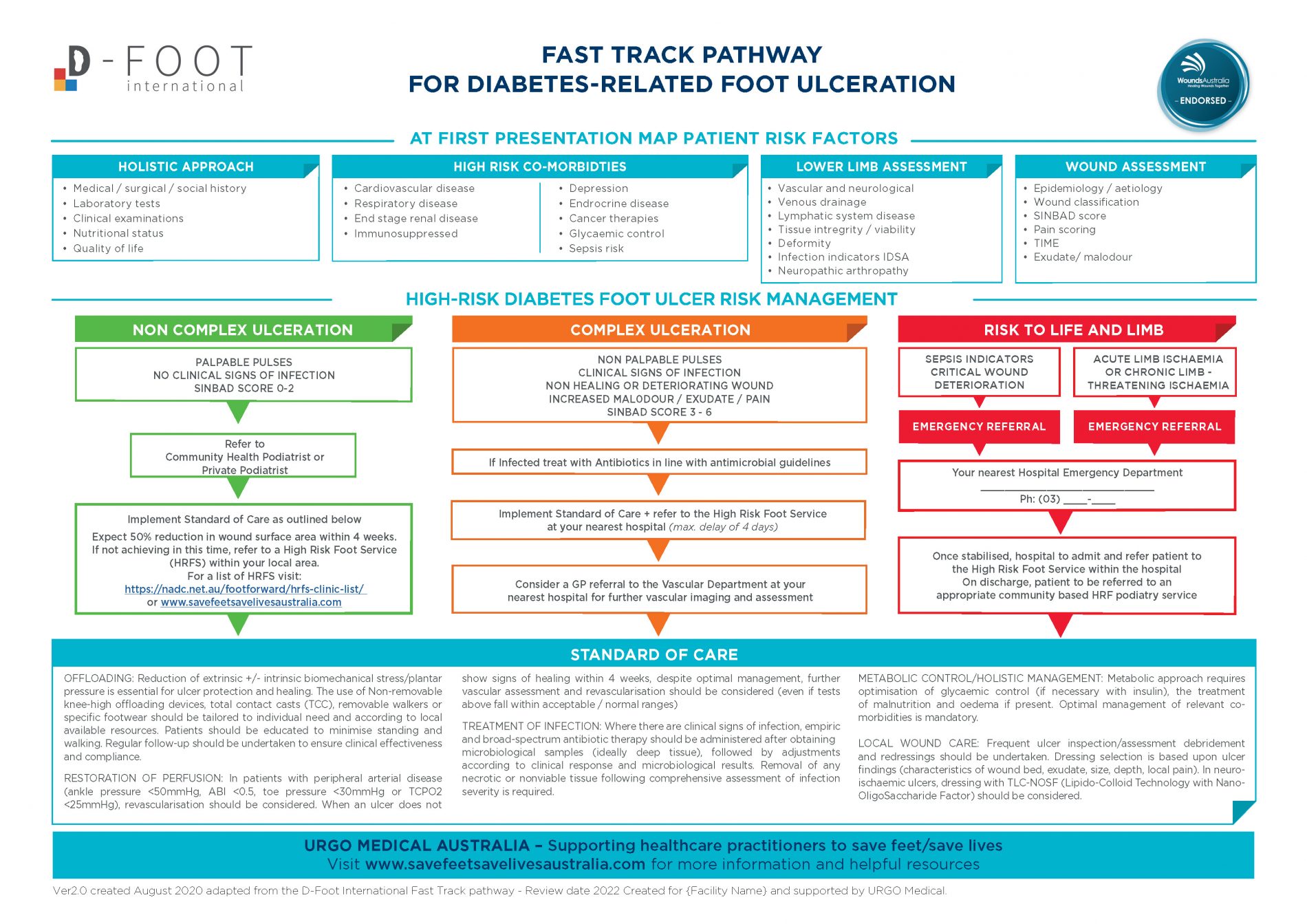
This is the recommended standard of care2 that will be put in place by the multidisciplinary team in a specialised setting.
OFFLOADING:
Reduction of extrinsic and/or intrinsic biomechanical stress/plantar pressure is essential for ulcer protection and healing. The use of non-removable knee-high offloading devices, total contact casts (TCC), removable walkers or specific footwear should be used tailored to individual need and according to local available resources. Patients should be educated to minimise standing and walking. Regular follow-up should be undertaken to ensure clinical effectiveness and compliance.
treatment of infection:
When there are clinical signs of infection, empiric and broad-spectrum antibiotic therapy should be administrated after obtaining microbiological samples (ideally deep tissue), followed by adjustments according to clinical response and microbiological results. Removal of any necrotic or non-viable tissue following comprehensive assessment of infection severity is required.
metabolic control / holistic management:
Metabolic approach requires optimisation of glycaemic control (if necessary with insulin), the treatment of malnutrition and oedema if present. Optimal management of relevant co-morbidities is mandatory.
restoration of foot perfusion:
In patients with peripheral arterial disease (ankle pressure <50mm Hg, ABI <0.5, toe pressure <30mmHg or Tcp02 <25 mmHg), revascularisation should be considered. When an ulcer does not show signs of healing within 4 weeks, despite optimal management, further vascular assessment and revascularisation should be considered (even if the tests above fall within acceptable/normal ranges).
local wound care:
Frequent ulcer inspection/assessment, debridement and redressings should be undertaken. Dressing selection is based upon ulcer findings (characteristics of wound bed, exudate, size, depth, local pain). In case of neuro-ischemic ulcers, dressings with TLC-NOSF (Lipid-Colloid Technology with Nano-OligoSaccharide Factor) should be considered.
Remember
Make sure that your patient gets the appropriate level of care depending on their level of risk, even if there is no wound.
learn more
How to identify the Loss of Protective Sensation (LOPS)
Performing a sensory foot examination will help you identify the degree of Loss of Protective Sensation (LOPS).
Ideally use a 10g (5.07 SemmesWeinstein) monofilament
Download tips & tricks1. Meloni M, Izzo V, Manu C et al (2019) Fast-track pathway: an easy-to-use tool to reduce delayed referral and amputations in diabetic patients with foot ulceration The Diabetic Foot Journal 22(2): 38–47
2. IWGDF- Guidelines on the prevention and management of diabetic foot disease – 2019.